Being a sex journalist whose work often has a psychological bent, I’ve read many a research study in my time. Usually I’m just combing these PDFs for facts to bolster my argument, but occasionally I find one so consumingly weird or interesting that I read the whole thing, agog – like that time I live-tweeted reading Dr. Chua Chee Ann’s groundbreaking study in which he “discovered” the anterior fornix.
I had one such experience recently when, combing through theories of fetish formation as research for a client project, I stumbled across a case study from 1954 detailing the wild woes of a man with an unusual fetish. Buckle up; let’s get into it…
The study opens by introducing us to our protagonist, a 38-year-old man who suffers from both epilepsy and a lifelong fetish for safety pins – specifically, “bright shiny” safety pins. I say “suffers” here not because fetishes are inherently bad (they’re not) but because his interferes with his relationship, as we’ll see later. In spite of this, he admits that looking at safety pins gives him what he calls a “thought satisfaction” that is “the greatest experience of his life – ‘better than sexual intercourse.'”
If you’re wondering where his epilepsy comes into all of this, here it is. The man, the study goes on to say, started to notice “blank periods” of memory when he looked at safety pins starting at around age 8, but because he would always retreat to the privacy of a bathroom before indulging in this carnal habit, no one ever actually observed him blanking out until his wife did when he was 23. On subsequent viewings, it became clear that looking at safety pins reliably brought on some kind of epileptic episode for this man: he would look at the pin for a minute, go glassy-eyed, make humming and sucking noises with his lips, and sometimes walk backwards “while his right hand plucked at his left sleeve.” For all this time, he would be unresponsive. Sometimes this type of episode also induced “postictal confusion” severe enough that he would dress himself in his wife’s clothing afterward, the study mentions offhandedly. (Was he into crossdressing too, or was he just disoriented?! The world may never know.)
To dig even more deeply into this poor man’s sex life… He most often felt the urge to look at a safety pin during “sexual stimulation and anxiety-producing situations,” which gels with my experience of my own kinks: I think about them when I’m turned on, sure, but also when I’m stressed out and seeking comfort. Occasionally he would have an epileptic fit of the aforementioned sort if he fantasized about safety pins during sex or masturbation, suggesting, interestingly, that it was the thought of pins moreso than the reality of them that induced these episodes. (But then, aren’t our kinks always “all in our heads,” fundamentally?) In classic 1954 fashion, the study notes, “Most frequently the fits occurred soon after awakening when, with a full bladder, adult sexual outlets were sought but refused by a frigid wife.” (Dude, you’d probably act “frigid” too if your husband had a unique fetish in a world lacking proper sex education and kink-positivity. Yeesh.)
Also standard for the 1950s, the study goes on to blame the man’s “over-affectionate mother” for him being “effeminate.” In the same section, it describes his childhood habit of collecting and playing with safety pins. Apparently, on one occasion, he clearly saw a safety pin in his mother’s discarded underclothes, an event which my inner fetish detective wants to guess is the origin of his kink, but we can never know for sure.
In detailing his sex life during adulthood – which is relevant insofar as a psychological “aberration” like a fetish is often only considered a problem if it causes the patient distress or impairment in their life – the study mentions that he has “voyeuristic tendencies, with emphasis on women’s breasts,” suggesting that he has at least some sexual interests outside of safety pins. However, it goes on to say that within the last five years he has increasingly suffered from impotence, “claiming that the safety pin had replaced his need for a genital outlet.” This, we might reasonably call an impairment – though it depends on your understanding of what a healthy sex life is, doesn’t it?
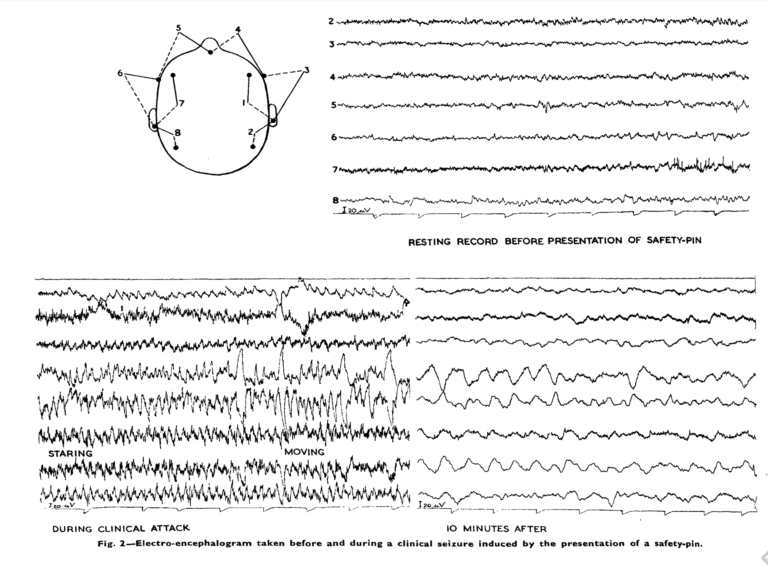
In any case, the epileptic fits (if not the fetish itself) had evidently caused the man sufficient distress that he sought treatment. (He’d also experienced a few episodes of psychosis, presumably epilepsy-related, in which he believed himself to be a relative of the king or a messenger of God.) After confirming epileptic activity with brain tests in the lab, both before and after showing him safety pins, doctors surgically removed the part of his anterior temporal lobe that the tests had determined were the problem area.
16 months after surgery, the man came back into the hospital for a follow-up. Amazingly, he reported he had had no further epileptic fits and no further desire to look at safety pins. His boner issues had even resolved; he was now able to have a full and satisfying sex life with his (frigid??) wife. Further brain tests were done and confirmed that, unlike before the surgery, nothing major changed in his brain activity when he looked at a safety pin. The fetish was effectively gone.
Reading this study left me with the question: Is it good – morally, practically, or otherwise – to take away someone’s fetish if it’s causing them consternation? Obviously there are cases where reducing or removing a particular aberrant desire is arguably necessary for the greater good, like when pedophiles with a history of committing sexual assault are chemically castrated; I’m not totally sure how I feel about these measures, but many healthcare professionals and even some pedophiles themselves think this is the best option. In cases where a fetish isn’t causing harm, however – or is only causing harm insofar as it’s stigmatized and creates friction in the fetishist’s relationships and/or self-image – can we really say it’s “good” to take away the locus of someone’s passionate desire?
Like the kinky equivalent of conversion therapy, many methods have been suggested for “removing” people’s kinks from their brains. But also like conversion therapy, it seems to me that this line of thinking only comes up because we live in a world that so deeply stigmatizes some people’s perfectly acceptable desires. Who is harmed by this man having a safety pin fetish? Maybe his wife, who wanted a better and more conventional sexual connection with her husband – but perhaps then she should’ve picked a different partner, or learned how to use his fetish to arouse him during sex. Maybe he himself is harmed, in that he felt inadequate and weird because of his fetish – but arguably that’s just a function of cultural kinkphobia. Both of these people were probably just trying their best, within a time period that severely limited the ways one could think about fetishism – but this attitude often still persists today, at a time when we’re much better-equipped to handle and think about fetishes, and it’s sad.
While I’m glad that the man in this study was seemingly cured of his epileptic episodes, I wish he had been able to hang onto his fetish – without it upsetting him or troubling his relationship. Looking at safety pins, after all, was “the greatest experience of his life,” even if he no longer cared to do it after his surgery. It saddens me to think that anyone could see that type of exquisite “thought satisfaction” as anything less than healthy, wonderful joy.